

Expose the whole lower leg and foot.
Examine the soles of the patient's shoes for signs of asymmetrical wear
Look for side to side asymmetry or abnormal contact w/ the ground
Walking Gait - look for a high stepping gait (foot drop, equinovarus), antalgic gait (ankle, hindfoot or midfoot pain) and short propulsive phase (forefoot pain)
Look at the patient standing (and then sitting).
- Limb alignment (especially genu valgus with flat feet)
- Look at the foot shapes and positions.
- Medial arch - obliterated in pes planus, exaggerated in pes cavus (NB - look at lower back for signs of spina bifida or neurofibromatosis)
- Hindfoot (from behind) - varus (pes cavus) or valgus (pes planus). Ask patient to stand on tiptoes and see if deformity corrects (= mobile subtalar joint).
- 'Too many toes' sign = looking from behind more toes are seen on the lateral side of the leg. This occurs in pes planus, splayed forefoot.
The patient should sit on the examination couch with both lower legs hanging over the side. The examiner should sit on a chair at a lower level than the couch.
Overall Foot Shape:
- neutral or rectus foot - no overall deformity
- flat foot - heel valgus, low arch, commonly forefoot abduction and supination. The subtalar joint is commonly in the overpronated position in stance and may be even more so on walking. Distinguish between flexible and rigid flat feet by asking the patient to stand on tiptoe to see if the arch re-appears and the heel goes into varus. Then do a single foot tiptoe test to look for tibialis posterior insufficiency. The "too many toes sign" demonstrates forefoot abduction. Manipulate the subtalar joint to identify a rigid hindfoot suggesting arthritis or a tarsal coalition. Exclude a neurological cause by appropriate examination.
- cavus foot - typically with a plantar flexed first ray, high arch and forefoot pronation. In many cases the hindfoot is in varus and this may be fixed or mobile. Use the Coleman block test to tell the difference. Pes cavus may be associated with spinal anomalies (especially if asymmetrical) or with hereditary sensorimotor neuropathies such as Charcot-Marie-Tooth disease.
- skewfoot - hindfoot valgus and forefoot adduction. Do the same tests for hindfoot correction as in flatfoot. Manipulate the forefoot to determine correctability of adduction.
- metatarsus adductus - neutral hindfoot and adduction of the metatarsus (some patients have some forefoot supination too). Commonly seen in pre-school children when it is usually correctable, but also in adults when it is often relatively fixed but usually in itself asymptomatic.
Look at the:
- Skin on the Dorsum and Plantar surfaces
- Muscle wasting
- Nail condition and hygiene
- Bony prominences or exostoses
- Check Dorsalis Pedis & Posterior Tibial Pulses
- Ask for & feel the tender area
ANKLE
Feel for tender areas, systematically checking:
- the anterior joint line
- the lateral gutter and lateral ligaments
- the syndesmosis
- the posterior joint line
- the medial ligament complex
- the medial gutter
Feel for an effusion, synovitis, deformity, bony prominence and loose bodies.
HINDFOOT & MIDFOOT
Palpate the following structures from Lateral to Dorsum to Medial surfaces:
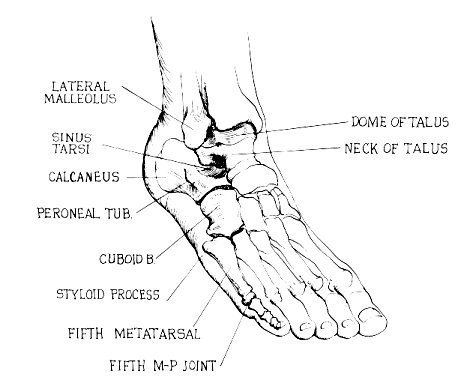
Lateral (from distal to proximal) [Figure 1] :
- Styloid process of fifth metatarsal
- Groove in the cuboid for Peroneus Longus tendon (just posterior to 1)
- The peroneal tubercle (a small lateral extension of the calcaneus, separating the peroneus longus & brevis tendons)
- Sinus Tarsi - soft tissue depression just anterior to the lateral malleolus. (Sinus Tarsi is filled with EDB & fat pad)
Dome of Talus (made prominent by plantarflexing ankle)

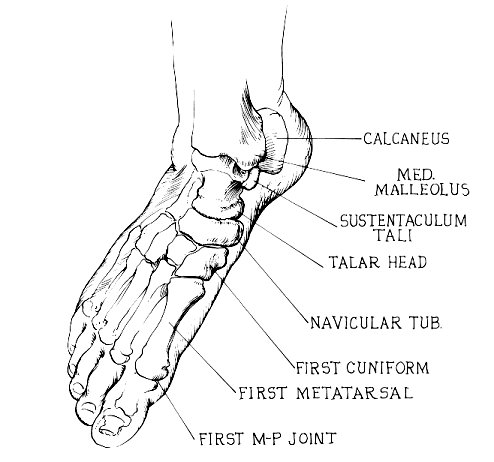
Medial (from proximal to distal) [Figure Below]:
- First Metatarso-cuneiform joint.
- Navicular Tubercle - most obvious bony prominence in front of medial malleolus. (insertion of Tibialis Posterior tendon)
- Head of Talus - felt just behind the navicular, by everting & inverting the midfoot.
- Sustentaculum Tali - one fingerbreadth below medial malleolus. (serves as an attachment for the spring ligament & supports the talus)
- Medial Malleolus.
FOREFOOT
Palpate the all bones and joints in a circle, paying particular attention to:
- First Metatarsal head
- First MTPJ
- Metatarsal heads
- Web spaces
PAED | P ronation = A bduction, E version & D orsiflexion |
SAPI | S upination = A dduction, P lantarflexion & I nversion |
Compare both sides
Active Combined - ask the patient to lift foot up (dorsiflex) and down (plantarflex)
Passive -
Dorsiflexion = Put one hand on the heel with the same forearm supporting the foot. The other hand supports the tibia. Dorsiflex the ankle by lifting the forearm under the foot. [Figure Below] (Normal = 55 degrees)

Plantarflexion = As in [Figure Below] below: (Normal = 15 degrees)

Hold the calcaneus with one hand and the talar head/neck with the thumb & index finger of the other hand. Apply varus and valgus stress with the hand on the calcaneus feeling for movement of the talus (at extremes of subtalar motion) with the other hand. Holding talus rather than the tibia isolates subtalar from ankle motion. (Normal = 5 degrees in each direction)
The subtalar joint can also be examined with the patient prone & the foot off the end of the couch.
MIDTARSAL (Talo-navicular & Calcaneo-cuboid joints)
Hold the calcaneus with one hand and move the forefoot medially & laterally with the other hand = adduction (20 degrees) & abduction (10 degrees). This movement cannot be seen, but can be felt.
Active motion is zero, but test the joints for stability (by pushing each joint up & down)
FIRST METATARSOPHALANGEAL JOINT
Normal ROM = 70-90 degrees DF; 45 degrees PF. Normal toe-off requires 35-40 degrees DF.
TIBIALIS POSTERIOR MUSCLE & TENDON
From behind, ask the patient to do a single foot tiptoe test on both sides. Most people cannot get the affected heel off the ground at all; a few develop an acute midfoot breach. Another useful test is to get the patient to contract the tibialis posterior in the plantar-flexed/inverted position. The tendon may be weak, impalpable or palpably thin. Always examine for an Achilles contracture which is present in most people with tibialis posterior insufficiency and may only be apparent with the heel held in neutral or varus.
TIBIALIS ANTERIOR MUSCLE & TENDON (L4,5)
Ask the patient to walk on his heels with his feet inverted. The tibialis tendon can be seen prominent.
Manual test = the patient should sit on the edge of the examination table. Support his lower leg, and place your thumb near the dorsum of his foot in such a position that he must dorsiflex and invert his foot to reach it. Test resisted eversion from this position. Palpate the tibialis anterior muscle as you perform the test.
PERONEALS
Ask the patient to walk on the medial border of his feet.
Manual test = Secure the ankle by stabilising the calcaneus and with the other hand feel the peroneal tendons while testing resisted eversion. (Reverse of the Tibialis Anterior test)
Peroneal Snapping = DF & PF the ankle with the foot everted and palpate for 'snapping' of the peroneal tendons over the lateral malleolus
ANKLE
Test for ankle stability using the anterior draw and tilt tests. In the acute trauma situation pain makes these difficult. Sometimes local anaesthetic injection into damaged ligaments or the lateral popliteal nerve makes stress testing easier. When doing the tilt test, hold the talus at the neck, rather than the heel, as then you can be sure that any tilt is in the ankle not the subtalar joint. Instability of the syndesmosis may be palpable, usually on A-P translation of the distal fibula or valgus stress of the ankle.
OTHER TESTS
DISTAL TIBIO-FIBULAR JOINT / SYNDOSMOSIS
FIBULAR DRAW TEST
When attempting to displace the fibula anteriorly in an uninjured ankle, the examiner cannot elicit movement; - in a normal ankle the examiner frequently can feel movement when he attempts to displace the fibula posteriorly; - rarely can he initiate an increase in anterior displacement of the fibula in pts who have sustained injures to the ligamenotuos structures supporting the syndesmosis; - w/ sprain, the examiner can initiate increase in posterior displacement which usually reproduces pain;
CORONAL DRAWER TEST
talar motion in the coronal plane is another indication of syndesmotic widening.
SQUEEZE TEST
clinical test for syndesmotic instability; - w/ positive test, compression of the proximal calf causes pain at the distal syndesmosis; - anatomically, squeezing the proximal calf will cause separation of the distal fibula and specifically will cause separation of the anterior tibiofibular ligament
Note the position of the heel when standing on a 2cm block. Then get the patient to stand with the forefoot over the medial edge. If a varus remains then the subtalar joint is fixed. If it corrects to valgus then the joint is mobile.
ACHILLES TENDON TEST (Simmonds / Thompson)
Lie the patient prone and squeeze the calf to elicit movement at the ankle = intact TA.
3 komentar:
This seems easy. I could apply it fast.
osteo arthritis
nic..sir
you can also cheak my site about all footwear design
Posting Komentar