

Definition
Disorder of movement and posturing
Caused by static brain lesion
Acquired during the stage of rapid brain development
Manifestations may change with growth and development
Occurs in 1-5 in 1 000 live births. More common in advanced countries. Advanced perinatal care increases survival of brain-damaged children. Care only slightly reduces incidence of cerebral palsy . More common in socioeconomically disadvantaged.
Aetiology Aetiology
Prenatal (30%)
Maternal infection - Toxoplasmosis . Rubella . Cytomegalovirus . Herpes . Syphilis
Maternal exposure - Alcohol . Drugs
Congenital brain malformations
Perinatal
Birth weight <2500g>(25-40%)
Anoxia (10-20%)
Postnatal (10%)
Meningitis
Head injury
Immersion
1. Spastic
Most common (60% of cases)
Most amenable to surgery
Due to upper motor neuron involvement - mild to severe motor impairment
Characterized by increased muscle tone and hyperreflexia, with slow, restricted movements (because of co contraction of agonist and antagonists)
Spasticity is characterized by increased muscle activity with increasingly rapid stretch (clasp knife & clonus)
Contractures
hemiplegia (both limbs on one side): arm usually worse than leg - all hemiplegics will walk, regardless of treatment; present with toe walking only
diplegia : have more extensive involvement of the lower extremity than the upper extremity; most diplegics will eventually walk; IQ may be normal, strabismus is common; gait is typically characterized by a crouched gait, toe walking, and flexed knees; heel cord lengthening alone may exacerbate crouched gait;
paraplegia (both legs): sparing of arms
quadriplegia : look for oral, lingual, dys f(x); dysarthria;
2. Athetoid / Dyskinetic
Writhing movements. When excited, wriggle as if tickled.
20% of cases
Result from basal ganglia involvement
Present w/ slow, writhing, involuntary movements
may affect the extremities (athetoid), or the proximal parts of limbs and the trunk (dystonic)
Hyperextended hips & knees with exaggerated stepping gait. Lean backwards, extending shoulder girdle & trunk.
Abrupt, jerky distal movements (Choreiform) also may occur;
Movements incr during with emotional tension and disappear during sleep.
Dysarthia is present and is often severe.
Intelligence normal (often above average)
Most difficult to correct with surgery - results are unpredictable & plaster immobilisation hazardous due to friction from constant movements.
3. Ataxic
10% of cases
Involvement of the cerebellum or its pathways
Weakness, inco-ordination, and intention tremor produce unsteadiness, wide based gait, and difficulty with rapid or fine movements
Poorly amenable to surgical correction;
4. Hemiballistic
Sudden movements . As if throwing ball.
5. Hypotonic
Usually a stage through which an infant passes.
6. Combination
1. Weakness
Upper motor neuron lesion causes
Loss of voluntary movement
Weakness
Easy fatigability
2. Spasticity
Feature of all lesions of pyramidal system . Cerebral, capsular, pontine, midbrain lesions
Related to excessive activity of disinhibited spinal neurones
Mediated via stretch reflex . Muscle spindles detect stretch and stimulate muscle to contract . Threshold regulated by descending tracts . Spasticity due to hyperactivity of stretch reflexes
Tendon reflexes hypertonic . Clonus may appear
Posture characteristic because some neurones more active than others
Attempts to change position lead to resistance which quickly yields Clasp-knife phenomenon.
3. Contracture.
Nature of muscle contracture is: Shortening of muscle-tendon unit due to failure to keep pace with growth of bones.
Muscle adds sarcomeres at musculotendinous junction in response to constant stretch
In normal children, walking and movement provide all the stretch needed. When muscles spastic, this mechanism cannot occur.
4. Deformity
From unopposed muscle contracture.
Hip dislocation. Persistent hip adduction leads to valgus of femoral neck. Persistent hip flexion leads to anteversion of femoral neck. Results in Acetabular dysplasia, Hip subluxation & Hip dislocation
Note:
Spasticity - Abnormally increased contraction of a muscle in response to a stretch. Growth of muscles is impaired.
Rigidity - Involuntary sustained contraction of a muscle not stretch-dependent. Growth of muscles is not impaired.
1. Spastic quadriplegia. (25%)
Initially child floppy and will not feed
Choking during feeding from pseudobulbar palsy (difficult swallowing & chewing; dribbling)
Fail to thrive
Intelligence, vision and hearing affected
Only 10-20% will walk
Begin to walk up to age 7
Usually mentally retarded
Develop hip dislocation early and scoliosis.
2. Spastic diplegia.(30%)
All developmental milestones delayed
Most walk by age 4 .
3. Spastic hemiplegia (40%)
Usually noticed at walking age
Mean age of walking is 2-3 months later than normal.
Limp and one-handedness noted
Right-sided form may have speech delay
Seizures common.
Mild learning problems
Hyperactivity
4. Monoplegia (5%)
Associated disorders
Most common with total involvement
Mental retardation
Seizures
Learning disorders
Emotional and personality derangement
Visual defects
Hearing impairments
Disorders of speech
History
Abnormal birth history
Prematurity
Neonatal nursery
Normal Developmental milestones (brackets are 95th percentile)
Head control -3 mths (6 mths)
Sitting independently - 6 mths (9 mths)
Crawling - 8 mths (never)
Pulling to stand - 9 mths (12 mths)
Walking -12 mths (18 mths)
Examination. (Also see CP Examination )
Walking- Arm swing . Trunk leans forward. Scissoring (d.t. Hip flexion & adduction). Windswept posture . Knee flexion . Stride length reduced . Narrow walking base. Equinus. Lordosis . Co-ordination in turning. [ Gait Analysis ]
Sitting - Legs forward or W . Upright or slouched.
Kneeling eliminates contracture effect .
Hips - Clinical signs of dislocation:
Limited abduction, esp. with rapid stretch (grab test)
Asymmetric knee height with pelvis level & knees flexed ( Galeazzi test )
Windswept posture - one hip adducted & other side abducted
Asymmetric leg length
Hip flexion contractures
Muscles:
Psoas
FFD of hip demonstrated by Thomas test
Increased lumbar lordosis and prominent bottom when standing
Decreased sacrofemoral angle on standing lateral x-ray
Reduced SLR because of flexed pelvis from FFD.
Hamstrings
Reduced SLR
Hip extension contracture
FFD at knee
Lumbar kyphosis and small bottom when standing
Knee flexed at beginning of stance phase
False equinus (flexed knee lifts heel from ground)
Internal femoral torsion (sitting in W position)
Inability to touch toes
Reduced popliteal angle (hip at 90o)
High patella (flexed knee and spastic quadriceps)
Adductors
Scissored gait if bilateral
Apparent leg length discrepancy if unilateral
Trendelenberg limp
Decreased hip abduction
Eventual hip dislocation
Quadriceps
Stiff-legged gait (knees never flex)
Inability to flex knee when hip extended means rectus is responsible
Ely test (child prone, flex knee, if hip flexes = rectus femoris tight).
Triceps surae
Ankle equinus
Tiptoe gait
Recurvatum at knee when heel goes down
Silverskold's Test - equinus improves with knee flexion = soleus tighter than gastrocnemius
Neurology
Gross. Weakness
Clasp-knife phenomenon
Primitive reflexes
Moro reflex - Hold child at 45 o . Allow head to drop back . Arms and legs stick out in extension . Normally disappears by 4 mths.
Labyrinthine reflex - Tone reduced and arms and legs flex when child prone . Tone increased and arms and legs extend when child supine . Normally disappears by 6 mths.
Parachute reflex - When child held head down, both hands put out protectively . Appears at 5 mths.
Upper limbs
General.
Look at resting position.
Look for contractures.
Assess joint stability
Hand placement. Ask patient to place hand on knee and then head.
Control.
Ask patient to pretend to play piano . Look for independent movement.
Ask patient to throw object. Look for grasp and release.
Stereognosis. Test ability to recognise shape in palm
Predictors of Walking (from 1 year of age):
Asymmetrical tonic neck reflex
Symmetrical tonic neck reflex
Neck righting reflex
Moro reflex
A pattern of extensor thrust & abduction of the legs when supported upright
Parachute reflex
Stepping reflex
If any 2 of these 7 responses are inappropriate by 1 year of age it is highly unlikely that the child will walk independently




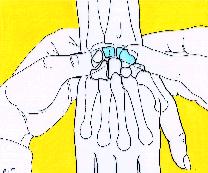 Scapholunate Ballotment Test
Scapholunate Ballotment Test 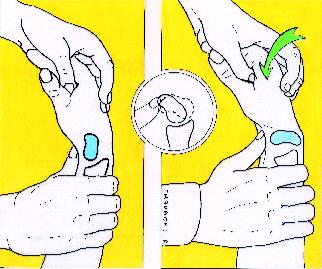 Kirk-Watson Test
Kirk-Watson Test 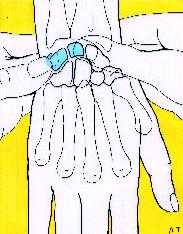 Reagan Test
Reagan Test  Kleinman Shear Test
Kleinman Shear Test